Aug 12, 2025
15
mins read
Hepatitis D – also known as hepatitis D virus infection or delta hepatitis – is a viral infection that causes inflammation of the liver and occurs only in people who are already infected with hepatitis B virus (HBV). Hepatitis D virus is a defective virus that depends on HBV for its life cycle, making it a unique satellite virus. It is considered the most severe form of viral hepatitis in humans, leading to faster progression to liver fibrosis (scarring), cirrhosis, and liver cancer than HBV infection alone. Global estimates indicate that roughly 5% of chronic hepatitis B patients (about 12–20 million people worldwide) are co-infected with hepatitis D. This dual infection is a growing public health concern, as hepatitis D disease markedly worsens patient outcomes.
Why is Hepatitis D Virus (HDV) Classified as Cancer-Causing?
Worsens HBV Outcomes: Co-infection increases liver cancer risk by 2–6 times vs. HBV alone.
Rapid Liver Damage: Up to 75% develop cirrhosis in 15 years, compared to 50% in HBV-only cases.
Aggressive Progression: Fast-tracked development of fibrosis and liver failure in younger populations.
HDV hijacks HBV’s replication machinery, amplifying viral and oncogenic load.
The World Health Organization (WHO), via the International Agency for Research on Cancer (IARC), recently classified hepatitis D virus (HDV) as carcinogenic to humans (Group 1), alongside hepatitis B and C. This reclassification highlights hepatitis D’s strong link to liver cancer (HDV infection increases liver cancer risk 2–6 times compared to hepatitis B alone) and underscores the urgency of preventing and managing this viral hepatitis D infection.
Table of content
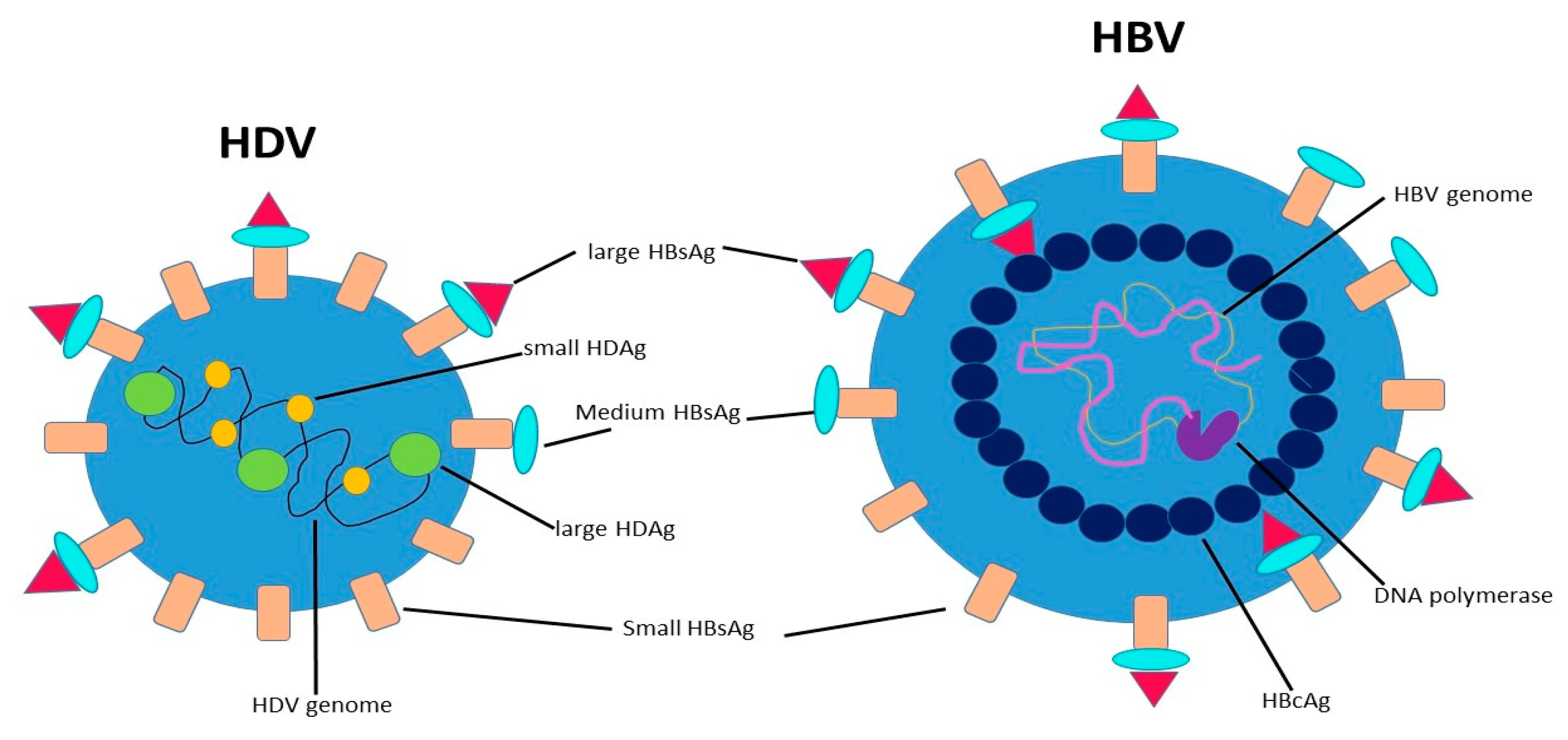
Defective Virus:
Hepatitis D virus is a single-stranded RNA virus that is “incomplete” and requires HBV to replicate and infect liver cells.
It cannot infect on its own; Hepatitis D virus piggybacks on hepatitis B, using HBV’s surface proteins to assemble new virus particles.
Delta Hepatitis:
Hepatitis D is often called delta hepatitis. Infection by Hepatitis D virus only occurs in people with hepatitis B – either at the same time (co-infection) or in someone with an existing chronic Hepatitis B infection (superinfection).
If a person is not infected with HBV, they cannot contract hepatitis D.
Most Severe Hepatitis:
HDV causes the most severe form of viral hepatitis known. Co-infection with HBV leads to more aggressive liver disease than HBV alone, accelerating progression to cirrhosis, liver failure, or cancer.
WHO notes that only hepatitis B, C, and D can cause chronic infections with high risk of cirrhosis and liver cancer.
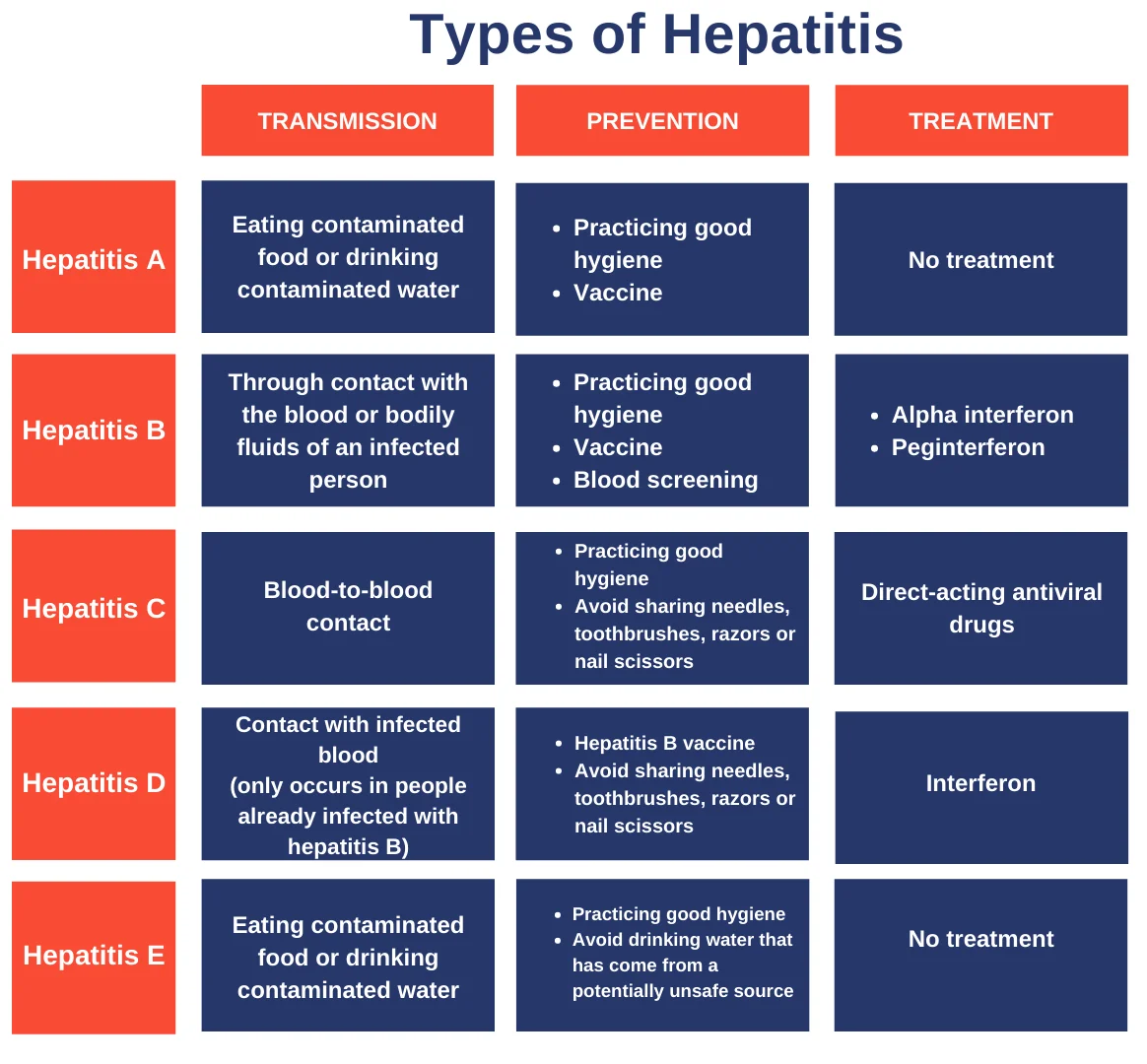
Mode of Transmission:
Hepatitis D spreads in the same ways as hepatitis B – through contact with infected blood or body fluids
Key routes include
contaminated needles (e.g. injecting drug use, unsafe injections),
blood transfusions with unscreened blood,
unprotected sexual contact, and from an infected mother to child during birth (vertical transmission).
Acute Infection Symptoms:
In acute hepatitis D (when Hepatitis D virus is acquired, often as a co-infection), symptoms typically appear 3–7 weeks after exposure and are similar to other acute viral hepatitis symptoms, often more severe.
Common signs include:
Jaundice: Yellowing of skin and eyes.
Fatigue and Fever: Extreme tiredness, low-grade fever.
Gastrointestinal Issues
Dark Urine & Pale Stool: Dark-colored urine and clay-colored stool.
Joint Pain:
Body aches or joint pain can occur.
These symptoms indicate acute liver inflammation, it may lead to fulminant hepatitis (acute liver failure) requiring urgent care.
Chronic Hepatitis d Infection Symptoms:
In chronic hepatitis D (persistent infection, usually from HDV superinfection), many patients remain asymptomatic or have mild non-specific symptoms for years.
The liver damage accumulates silently. Often, no obvious symptoms appear until complications (cirrhosis or liver failure) develop.
At that late stage, signs may include chronic fatigue, abdominal swelling (ascites), leg swelling (edema), easy bleeding, weight loss, confusion (encephalopathy), or other symptoms of liver cirrhosis.
Feature | Acute Hepatitis D | Chronic Hepatitis D |
Definition | A short-term hepatitis D infection (<6 months), part of hepatitis D disease caused by hepatitis D virus (HDV). | A long-term viral hepatitis D infection (>6 months), almost always in patients with chronic hepatitis B virus (HBV) infection. |
Cause/Onset | Usually occurs in co-infection scenarios when HBV and HDV are contracted together. | Often occurs via superinfection – hepatitis D virus infecting an existing hepatitis B virus carrier. |
Immune Response | Strong immune response may clear both HBV and HDV; leads to full recovery in many cases. | Immune system unable to clear HDV due to persistent HBV, leading to chronic hepatitis D disease. |
Liver Damage | Minimal if cleared; fulminant hepatitis possible in severe cases. | Rapid fibrosis, cirrhosis, and high risk of liver failure or hepatocellular carcinoma. |
Severity | Can be severe in acute phase but potentially reversible. | Most aggressive chronic viral hepatitis; leads to severe complications without treatment. |
Diagnosis | Hepatitis diagnosis confirmed by HDV antigen/antibody tests and HDV RNA PCR in HBV-positive patients. | Same hepatitis diagnosis methods, with emphasis on monitoring liver fibrosis and cancer risk. |
Prevention | Hepatitis prevention via HBV vaccination is also prevention of hepatitis D. Avoid contact with infected blood/body fluids. | No HDV vaccine; prevention of hepatitis D disease through lifelong HBV control and avoiding high-risk exposures. |
Dependency on HBV: HDV entirely depends on hepatitis B virus – so an HBV infection is the foundation that allows HDV to exist. Both viruses infect liver cells, but HDV “borrows” HBV’s surface antigen (HBsAg) to assemble new viral particles. Thus, controlling HBV also suppresses HDV spread.
Mutual Impact: When HDV is present along with HBV, it tends to suppress HBV replication to some extent (HDV can out-compete HBV in liver cells). However, the combined infection causes more severe liver inflammation. HDV’s presence leads to worse clinical outcomes for HBV patients – including faster progression to cirrhosis and significantly higher cancer risk. In essence, HDV “piggybacks” on HBV but makes the overall hepatitis much more destructive.
Carcinogenic Synergy:
Chronic hepatitis B infection on its own can cause liver cancer (even without cirrhosis, as HBV DNA can integrate into host cells’ DNA).
When HDV is added, the carcinogenic effect is amplified. WHO and IARC note that hepatitis D co-infection increases the chance of liver cancer 2–6 fold compared to HBV alone.
This synergy is why hepatitis D is now recognized as cancer-causing in humans.
WHO Goals:
The WHO has set ambitious targets to eliminate viral hepatitis as a public health threat by 2030 (part of Sustainable Development Goal 3.3). The Global Health Sector Strategy (2022–2030) aims to reduce new viral hepatitis infections by 90% and mortality by 65%.
This includes hepatitis D through its dependence on hepatitis B control.
Every year on World Hepatitis Day (28 July), WHO reinforces calls for hepatitis prevention, testing, and treatment scale-up.
IARC Classification Impact:
With Hepatitis D Virus now officially classified as cancer-causing, global health agencies are raising awareness for better screening and surveillance of hepatitis D.
This may drive more resources into HDV testing (especially in hepatitis B carriers) and into developing HDV-specific treatments.
National Viral Hepatitis Control Program (India):
India launched the NVHCP in 2018 to combat hepatitis. Its goals include eliminating hepatitis C by 2030 and reducing morbidity and mortality from hepatitis B and D.
Strategies involve increasing hepatitis B vaccination, screening high-risk populations for HBV/HCV/HDV, and providing free treatment for hepatitis.
Despite programs, there are significant challenges: Low diagnosis rates – globally, only ~13% of HBV and 36% of HCV infected people were diagnosed by 2022 (HDV diagnosis is often even lower because it requires HBV patients to get an extra test).
Poor awareness and testing mean many HBV carriers don’t know their HDV status.
Vaccination gaps – in some countries, including parts of India, HBV infant vaccine coverage needs improvement (currently ~50% in India).
Also, limited treatment options and high costs (e.g., new HDV drugs) impede care.
Q1: Why is hepatitis D called a “defective” virus?
A: Because Hepatitis D Virus cannot replicate or infect by itself – it needs the hepatitis B virus’s presence and proteins to survive.
Q2: How is hepatitis D infection different from other hepatitis types?
A: Hepatitis D infection occurs only alongside hepatitis B and is the most severe hepatitis, causing faster liver fibrosis and higher cancer risk than other types
Q3: Can hepatitis D infection be cured completely?
A: Currently no definitive cure exists. Pegylated interferon can help some patients, and new drugs like Bulevirtide offer hope, but prevention via HBV vaccine is best.
Q4: What is the difference between co-infection and superinfection in hepatitis D?
A: Co-infection means getting HBV and HDV together (same time); superinfection means an HBV carrier later acquires HDV. Superinfection is more likely to become chronic (~90% cases) compared to co-infection (<5% cases).
Q5: Why has WHO classified hepatitis D as carcinogenic now?
A: Evidence showed HDV greatly increases liver cancer risk in hepatitis B patients. By classifying HDV as a Group 1 carcinogen, WHO/IARC aim to spur countries into improving HDV surveillance, prevention (HBV vaccination), and treatment access to reduce liver cancer deaths.
Q.6: What are the symptoms of hepatitis d virus?
A. Symptoms: Often asymptomatic initially, later fever, fatigue, loss of appetite, dark urine, pale stools, joint pain, jaundice.
Hepatitis D (HDV infection) is a critical public health issue due to its reliance on hepatitis B and its severe outcomes, including rapid progression to cirrhosis and liver cancer. The recent WHO/IARC classification of hepatitis D as carcinogenic underscores the need for heightened awareness, prevention, and research. For UPSC and civil services exam aspirants, understanding hepatitis D involves not only its virological link with HBV, but also the broader implications for public health policy – from vaccination programs to global health strategies. Strengthening hepatitis B vaccination and screening is the key to prevention of hepatitis D, while investment in new therapies offers hope for those already affected By eliminating hepatitis B, we can effectively eliminate hepatitis D in the long run, aligning with global goals of viral hepatitis control.
Internal Linking Suggestions
Tsunami UPSC, Meaning, Characteristics, Causes, Impacts & Mitigation Measures
How to Begin Your UPSC Preparation : The Ultimate Guide For Beginners
UPSC Previous Year Question Papers with Answers PDF - Prelims & Mains (2014-2024)
40 Most Important Supreme Court Judgements of India : Landmark Judgements UPSC
GST Council (Goods and Services Tax Council): Constitutional Provisions, Functions, Way Forward
External Linking Suggestions
UPSC Official Website – Syllabus & Notification: https://upsc.gov.in/
Press Information Bureau – Government Announcements: https://pib.gov.in/
NCERT Official Website – Standard Books for UPSC: https://ncert.nic.in
WHO official : who.int


